
What decides when you decide?
A clinical reframing of addiction as a problem of authority, not desire


Earlier I published an article introducing a simple but, I think, important idea: that addictive behaviour has a missing control variable. Specifically, at the point of decision, authority shifts to the object driving the action—most often the anticipated “high” and the relief that comes from resolving ambivalence.
Beyond “the high”: restoring self-governance at the point of decision

Most people who struggle with destructive urges already know the cost. They are not ignorant, and they are not stupid. Yet in certain moments, that knowledge disappears—and something else takes over. I argue that this “something else” is not vague or mysterious, but structurally identifiable: a
My sense is that this is a non-trivial advance for three reasons:
First, it identifies an upstream control variable—authority assignment—that existing models tend to leave implicit.
Second, it names a consistent failure mode: what appears to sustain the individual in the moment instead degrades their baseline over time (an inversion of the survival function).
Third, it provides a precise intervention point at the moment that matters—before the decision is effectively made.
In this piece, I have recast that insight into the form of a clinical briefing note. This is not because I am a therapist, recovery coach, or doctor, but because the pattern itself appears more general. It reflects a broader line of work I have been doing on governance and attribution, of which this is a particularly personal and immediate application. It is offered as a clarification of the idea, not as a claim of final authority or correctness.
The key takeaway is that existing approaches accurately describe the dynamics of addiction across biological, psychological, and social dimensions. What they tend to miss is the governance layer into which these mechanisms are embedded—specifically, what is granted authority to decide under conditions of incomplete attribution.
This piece can therefore be read at two levels:
as a practical intervention for addictive and self-sabotaging loops, and
as an instance of a wider class of failures in self-governing systems.
Authority Assignment at the Point of Decision in Addiction
A Clinical Briefing Note
March 2026
Important note
This is a conceptual refinement, not an empirically validated protocol. It is offered as a clinical thought partner to be integrated with your existing training, supervision, and ethical framework. Always use new interventions under appropriate supervision.
Summary
Contemporary models of addiction—spanning neuroscience, psychology, and therapeutic practice—provide robust explanations for craving, reinforcement, and behavioural persistence. These include:
Incentive salience theory (Berridge & Robinson): dissociation between “wanting” and “liking,” with sensitised cue-driven motivation
Allostatic / opponent-process models (Koob & Le Moal): progressive baseline degradation and negative reinforcement cycles
Dual-process frameworks: interaction between impulsive (automatic) and reflective (deliberative) systems
Clinical modalities (CBT/MI/ACT/MBRP): targeting cognition, behaviour, values alignment, and urge observation
[CBT = Cognitive Behavioural Therapy , MI = Motivational Interviewing, ACT = Acceptance and Commitment Therapy, and MBRP = Mindfulness-Based Relapse Prevention.]
These frameworks successfully describe:
The intensity and persistence of desire
The role of anticipation and relief in driving behaviour
The continuation of behaviour despite awareness of harm
However, they tend to treat behaviour as the outcome of competing internal processes without isolating a distinct upstream control variable—namely, what grants a given impulse the authority to determine action at the point of decision?
Proposed Refinement
Under conditions of cognitive or emotional load — here termed attribution debt (a temporary state in which the system cannot hold a sufficiently complete representation of downstream consequences) — the system substitutes a simplified construct in place of full outcome evaluation.
This construct is typically experienced as:
the anticipated “high,” or
the relief that comes from resolving ambivalence
Crucially, this construct functions not merely as a representation of reward, but as a decision-authorising object.
Key Distinction
Existing models describe misweighted valuation (e.g. immediate reward outweighs future cost)
This model proposes a misassignment of authority (a partial representation is treated as sufficient to decide)
This reframes the mechanism from an error in calculation to an error in governance.
The Inversion
A central implication is that the system can become misaligned with its own long-term viability:
The proxy is selected as if it sustains continuity (“this will stabilise me”)
The decision is subjectively experienced as correct
The outcome degrades baseline (energy, stability, resilience), increasing vulnerability
Thus, what presents as sustaining does not, in fact, sustain.
The anticipated improvement in baseline fails to materialise. Instead, the system returns more depleted, more vulnerable, and more dependent on the same construct it trusted.
This is the inversion:
the mechanism that appears to preserve continuity is redirected toward what undermines it.
Clinical Observation (Illustrative)
Clients often report a distinct shift immediately prior to relapse:
Once the decision to act is made, a sense of calm or relief appears
This occurs before any substance use or behavioural reward
The relief is interpreted as confirmation that the decision is “right”
In this model, that moment of relief represents the transfer of decision-making authority to the simplified construct, rather than the onset of reward itself.
Vignette 1 (chemsex loop) Client J (mid-30s) described: “The second I texted ‘on my way’, everything went quiet in my head. I felt calm for the first time all day — like the decision had already been made for me.” The substance hadn’t been taken yet. The relief marked the authority transfer.
Vignette 2 (binge-eating) Client S (late-40s) said: “The moment I decided to open the cupboard, the churning anxiety just… stopped. It felt like the right thing to do.” Again, the food hadn’t been eaten. The decision itself had been effectively deputised to the proxy.
Clinical Implication
The primary intervention point is not:
suppression of desire
correction of belief content
post hoc evaluation of consequences
Instead, the key task is restoring full attribution prior to authority assignment. In effect, the intervention does not oppose the desire, but changes the conditions under which it is allowed to decide.
This means reintroducing a complete representation of consequences before the simplified construct is allowed to determine action.
Operational Reframing
Replace:
“How will this feel?”
“Is this worth it?”
With: “What state will this leave me in?”
Focus shifts from immediate experience (“income”) to overall condition (“capital account”): energy, emotional stability, cognitive clarity, future vulnerability.
Example Micro-Intervention (one-breath version)
At the point of decision, prompt:
“Before you decide — if we fast-forward past the first ten minutes and look at tomorrow morning in your body, your head, and your options… where are you actually standing?”
This appears to:
interrupt premature resolution of ambivalence
prevent the simplified construct from being treated as sufficient
re-anchor decision-making in a broader temporal frame
Quick Integration with Existing Modalities
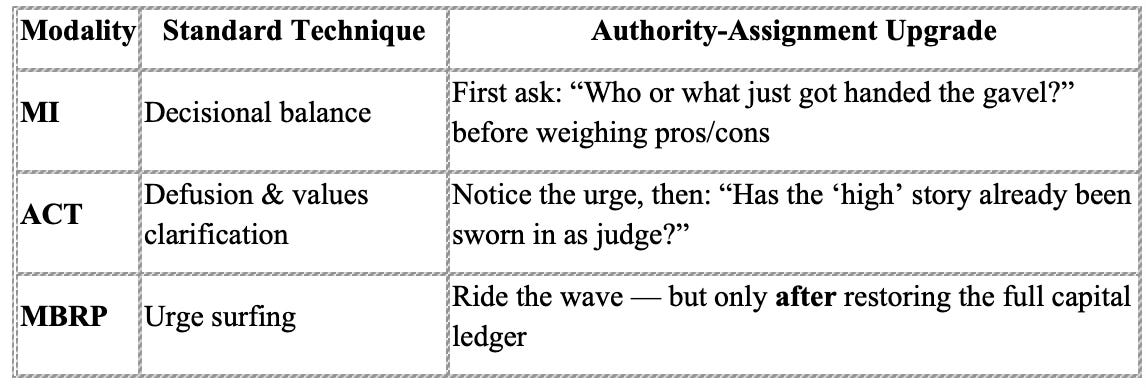
Client Handout (one-page version — ready to adapt)
“Before You Decide” Checklist Ask yourself (or your therapist):
If this fully plays out, where does it leave me tomorrow in my body?
In my mood and energy?
In my clarity and options?
In my relationships and future vulnerability?
Write the answers down. Then decide.
Positioning
This framework is not:
a new neurobiological mechanism
a replacement for existing therapeutic modalities
an empirically validated protocol
It is:
a higher-order organising principle integrating existing models
a proposal of an upstream control variable (authority assignment)
a phenomenologically grounded intervention point under real-time conditions
It may help explain why some established approaches struggle under high-load, in-the-moment scenarios: they operate downstream of the authority transfer.
Further Exploration
Potential areas for clinical and research investigation include:
Whether decision-relief reliably precedes reward as a reinforcing signal
Whether pre-decisional full-attribution prompts improve outcomes vs. standard techniques
How this framework integrates with trauma-informed and attachment-based care
Whether clients can be trained to identify and interrupt authority transfer in real time
Closing
This model suggests that addiction may be understood not only as dysregulated desire, but as a failure of self-governance under conditions of incomplete attribution.
Under these conditions, the system can select what appears to preserve it while producing the opposite effect.
Intervening at the level of authority—rather than behaviour alone—may offer a distinct and practical point of leverage in clinical work.
What this work points toward is a reframing of sovereignty and freedom. We all operate under constraints—sometimes severe ones, including coercion. The question is not whether we are constrained, but how we make decisions within those constraints.
At the point of choice, we can act on a fuller view of reality, or on a compressed substitute—a simplified proxy (“this will feel good”, “this will fix it”) that stands in for the whole. These shortcuts are not inherently wrong; they are necessary for functioning. The problem arises when they cease to be faithful summaries and become covers for omission—presented as sufficient when they are not.
In that sense, freedom is not the absence of constraint, but the capacity for self-governance: to act with sufficient visibility of consequences, rather than delegating the decision to a fragment that cannot carry the full weight of reality.
Once seen, the pattern is difficult to unsee. There is a recognition to it—something already half-known. What this work attempts to do is make that implicit understanding explicit, and therefore usable.
In retrospect, it feels obvious. But if it were truly self-evident, it would already be clearly articulated in the literature. It appears not to be. I offer it here in that spirit—for testing, refinement, and, if useful, application.